The UX of Death: End-of-life Literature Review
- Irene (Shiyin Zheng)

- Nov 29, 2018
- 6 min read
Updated: Jan 3, 2019
The UX of Death
Team
Cheuk Him Tam (Jordy)
Binghuai Chen
Yirui Fu (Floria)
Irene (me)
Artefacts Analysis Method
Mor taught us "Artefacts Analysis Method" in a workshop, which helps a lot when we have no ideas about how to design, especially in this abstract death project. It told us to go and find from one object and start from it. Find out more things about it and reach out the idea. Use it to think and even change it.
I grouped with Qin, Yaejing and Lara in the workshop. we were given the topic of "Ancient Greece".
Task 1: Pick an artefact and tell something about it
We were asked to think from the artefact, thinking about its value, material, quality, cultural meaning and so on. The coin is called Charon's Obol and it was used after people died. It would be put into the dead body's mouth or on his eyes. It was said to prevent the soul from coming out of the body. The coin was used to pay Charon, who was the ferryman of Hades. People in Ancient Greece believed people should go across the river after dying.
Task 2: Design something for a better death according to the artefact
The coin in Ancient Greece was used for dead body, and it was put into the dead body finally. The putting process was good because it felt like you were really doing something for him/her. It came to us that we could absorb this process into the funeral and design an interactive coin.
The coin could be passed from one person to another, everyone coming to the funeral could touch it and feel it just like feeling the passed-away person. The coin could also be heated up hand after hand, making it feel like the person's temperature. The person's family member would eventually get the coin and put it beside him/her, taking visitors' comfort to him.
I appreciate this idea much though it could still be developed. The coin could be designed into other kinds of medium. The interactive ways could be developed as well, not only the temperature. But these all started from the artefact. We got the idea in a so short time and the method really helped.


Development of the idea
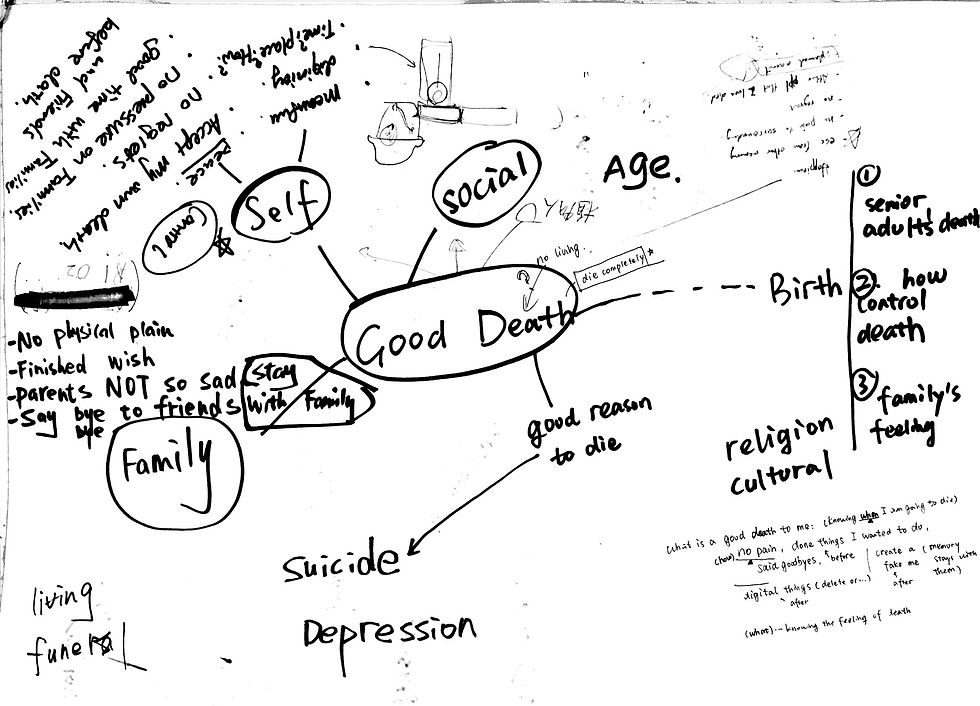
Death has been a distant topic for us and we started the discussion soon after the class. We talked about what is a "good death" in our thoughts. I advised that we all wrote our thoughts on the paper, and what we found interesting was that almost everyone of us mentioned a word "control". To us, a good death should be a controllable process - we should know when and how we were about to die. Another keyword was family. We cared about family's feelings a lot during death.
There are two ways of research, one is open research, and the other one is research after narrowing down topics. Taking into consideration the following week's design task, we agreed on deciding the topic first.
Speaking of our interest area, we chose "elderly" as our research target. Then we found both the "control" thing and the "family" thing were related with "emotions". So at first, our research on good death starts on these two keywords, "elderly" and "emotions".
However, we soon got stuck. The main reason was that there was just so little information on these two keywords and we seemed narrowed too much on the topic. We shared what we found in one google doc and rediscussed about the research direction and cleared up our mind. There are three stages of death, living (before death), dying and after death. The dying period was what we were focusing on. Through previous research, Jordy found one word "end-of-life decision", which was a controversial thing talked widely among the elderly. We started to focus on that thing and dig more out of it.
Literature Review
We divided this topic into four parts.
General definition of good death
A case in end-of-life period: “Terri Schiavo Case”
Conflicts among patients, physicians and families
Conflicts between people and society
I did literature review for the last part, conflicts between people and society. The most important one is law. Generally by law, when a patient is mentally capable, he or she must provide consent for the treatment decisions involved in his or her care. When the patient is not capable, a substitute decision-maker makes these decisions for the patient[1].
When a person is not capable, problems occur against the law. I concluded these into four arrows all pointing to the patient.
1 Different laws in different countries
Some patients would do advance directives before dying. And there is a DNR thing meaning do-not resuscitate order. But some countries do not have laws on these two things, resulting in more difficult decision making in some situations.
Some countries do not have laws on advance directives or DNR(do-not-resuscitate) orders, resulting in more difficult decision making in some situations.
For example, in Israel, withdrawal of life-sustaining therapies is not readily discussed, although withholding therapies is considered ethically acceptable[2].
2 Limitation of the judgement
Take Canada for an example. The ombudsman, who is an investigator from the government, cannot by law examine complaints about clinical judgement, and the clinical judgement means the decision of a clinician on a diagnosis or a particular course of treatment. However, the ombudsman can look at a range of other actions that result in poor care, like poor communication or poor administrative practices.
In Canada,It is important to note that the Ombudsman cannot by law examine complaints about clinical judgement, that is, the judgement of a clinician in deciding on a diagnosis or a particular course of treatment. The Ombudsman can however look at a range of other actions that often result in poor care, for example, poor communication, breach of procedure, or poor administrative practices[3].
3 Clinicians are confused about current law
Take England for eg.
Clinicians are confused about what decisions they can make. If a clinician want to withhold or withdraw treatment in patients in permanent VS and MCS, they have to look for court approval.
The current (somewhat anomalous) requirement for court approval to withhold or withdraw CANH in patients in permanent VS and MCS has left many clinicians confused about what treatment decisions they can make without reference to the court[4].
Current law: Practice Direction 9E of the Court of Protection (CoP) Rules describes court applications relating to serious medical treatments (2007). Section 5 states that ‘cases involving any of the following decisions should be regarded as serious medical treatment for the purpose of the rules and this practice direction, and should be brought to the court: (a) decisions about the proposed withholding or withdrawal of artificial nutrition and hydration from a person in a permanent VS (Vegetative state) or a MCS (Minimally conscious state)’[5].
Reason of the law:
The law is reasonable to some extent. Because in this kind of situation, death is unlike other medical decisions, it will inevitably occur within 2-3 weeks of CANH withdrawal (the withdrawal of clinically assisted nutrition and hydration), otherwise these patients might live for years. Therefore, these important order requires additional scrutiny.
Unlike other medical decisions that carry a certain element of chance, death will inevitably occur within 2–3 weeks of CANH withdrawal in a patient who might otherwise live for years. Therefore, it is considered that these decisions require additional scrutiny by the CoP in order to be declared lawful[6].
Some Argue:
But there are also some people(Keene) argue that the use of the word ‘should’ makes this a recommendation for good practice rather than a legal requirement[7].
4 Problems of law in practicality and ethics
Still, there are three main problems of the current law in England.
Time-consuming and expensive
A recent study from York the University of showed that the average time taken for this ‘declaratory relief ’ process in a VS case is about 9 months and costs to the National Health Service about £122 000 (comprising £53 000 in legal costs and £69 000 in ongoing care costs during the waiting period)[8].
Continuing treatment even during the process
While the court application is in process, clinical teams have sometimes been required by the Official Solicitor to provide further treatments that would otherwise have fallen above the planned ceiling of care[9].
Apply only to patients in permanent VS or MCS
Many patients would not live long enough for a judgement to be declared. Coma would not last for very long. Now doing decisions without reference to the court[10].

References
[1] College of Physicians and Surgeons of Ontario (2011). Decision-making for the End of Life. [online] Available at: http://www.cpso.on.ca/cpso/media/uploadedfiles/policies/policies/policyitems/end-of-life.pdf
[2] Thelen, M. (2005). End-of-Life Decision Making in Intensive Care. [online] Ccn.aacnjournals.org. Available at: http://ccn.aacnjournals.org/content/25/6/28.full#ref-16
[4] Turner-Stokes, L., 2017. A matter of life and death: controversy at the interface between clinical and legal decision-making in prolonged disorders of consciousness. Journal of medical ethics, 43(7), pp.469-475.
[5] Practice Direction 9E (2015). Serious Medical Treatment. Supplements. Part 9 of the COP rules 2007. [online] Available at: https://www.judiciary.gov.uk/publications/practicedirection-9e-applications-relating-to-serious-medical-treatment-effective-from-1-july-2015/ [accessed 12 Nov. 2016].
[6] Turner-Stokes, L., 2017. A matter of life and death: controversy at the interface between clinical and legal decision-making in prolonged disorders of consciousness. Journal of medical ethics, 43(7), pp.469-475.
[7] Keene, A.R., 2017. Procedure, practice and legal requirements: a commentary on ‘Why I wrote my advance decision’. Journal of medical ethics, 43(7), pp.435-438.
[8] Formby, A.P., Cookson, R.A. and Halliday, S., 2015. Cost analysis of the legal declaratory relief requirement for withdrawing Clinically Assisted Nutrition and Hydration (CANH) from patients in the Permanent Vegetative State (PVS) in England and Wales.
[9] Kitzinger, J. and Kitzinger, C., 2017. Causes and consequences of delays in treatment-withdrawal from PVS patients: a case study of Cumbria NHS Clinical Commissioning Group v Miss S and Ors [2016] EWCOP 32. Journal of medical ethics, 43(7), pp.459-468.
[10] Turner-Stokes, L., 2017. A matter of life and death: controversy at the interface between clinical and legal decision-making in prolonged disorders of consciousness. Journal of medical ethics, 43(7), pp.469-475.



Comments